

Abstract
Introduction: Venetoclax (Ven), an oral agent that targets the antiapoptotic protein, BCL-2, has demonstrated efficacy, as monotherapy and combined with proteasome inhibitor (PI) bortezomib, in relapsed/refractory (R/R) multiple myeloma (MM). We report preliminary safety and efficacy data for Ven combined with the second generation PI carfilzomib (K) and dexamethasone (VenKd) in R/R MM.
Methods: In this ongoing phase 2, dose escalation study (NCT02899052), patients with R/R MM and no prior K exposure received VenKd on 28-d cycles in 4 dose finding and one expansion cohorts: Ven 400 mg/day + K 27 mg/m2 Day 1, 2, 8, 9, 15, 16 + dex 40 mg Day 1, 8, 15, 22 (Cohort 1), same regimen but with Ven 800 mg/day (Cohort 2), Ven 800 mg/day + K 70 mg/m2 Day 1, 8, 15 + dex 40 mg Day 1, 8, 15, 22 (Cohort 3/expansion cohort), or Ven 800 mg + K 56 mg/m2 Day 1, 2, 8, 9, 15, 16 + dex 40 mg Day 1, 2, 8, 9, 15, 16, 22, 23 (Cohort 4). Treatment continued until progressive disease (PD) or unacceptable toxicity.
Results: As of June 11, 2018, 42 patients were enrolled. The median age was 66.5 years (min, max: 37, 79), 63% had ISS II/III disease, and 8 patients (19%) had t(11;14). Patients received a median of 2 prior therapies (range: 1 - 3), 93% had received prior PI (50% refractory), 62% were refractory to immunomodulatory therapies, and 33% double refractory.
At the data cut off, 29 patients were still active and had completed ≥2 cycles and 13 patients discontinued with the primary reason being disease progression (n=4), death (n=3), physician decision (n=2), withdrawal of consent (n=2), lack of efficacy (n=1), and AE (n=1). All patients experienced at least one AE, and grade 3/4 AEs experienced by >10% of subjects included: decreased lymphocyte count (26%), decreased neutrophil count (14%), and hypertension (12%). Thirteen subjects experienced at least one serious AE. Maximum tolerated dose was not reached and Ven 800 mg/day + K 70 mg/m2 was selected for expansion. Ven mean (% coefficient of variation) maximum plasma concentration (Cmax) and area under the plasma concentration-time curve over 24 hours (AUC24) on Cycle 1 Day 15 were 2.7 (57) mg/mL and 33.1 (54) mg×h/mL, respectively, at 400 mg venetoclax (n=4); and were 2.42 (53) mg/mL and 38.7 (51) mg×h/mL, respectively, at 800 mg venetoclax (n=13) in the dose escalation cohorts.
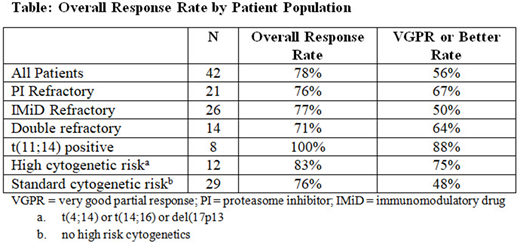
The overall response rate (ORR) was 78% and the very good partial response (VGPR) or better rate was 56% (Table). Median time from first dose to the data cut or discontinuation was 5.7 months (range: 0.9 - 16.3) and the median time to first response was 1.9 months (95% CI: 0.9, 9.2). ORRs for subgroups of interest are reported in the Table.
Conclusions: The combination of VenKd appears tolerable with no new safety signals or changes in Ven pharmacokinetics. VenKd shows promising preliminary efficacy in R/R MM patient subgroups. Response rates were comparable in all high risk subgroups and overall population. However, the subset of patients with t(11;14) had the highest response. Overall, these results demonstrate that VenKd is a safe and efficacious regimen in R/R MM and support the continued study of VenKd.
Costa:Abbvie: Research Funding; BMS: Research Funding; Karyopharm: Research Funding; Amgen: Honoraria, Research Funding; Sanofi: Honoraria; Celgene: Honoraria, Research Funding; Janssen: Research Funding. Stadtmauer:Celgene: Consultancy; AbbVie, Inc: Research Funding; Janssen: Consultancy; Takeda: Consultancy; Amgen: Consultancy. Morgan:Bristol-Myers Squibb: Consultancy, Honoraria; Janssen: Research Funding; Takeda: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding. Kovacsovics:Amgen: Honoraria, Research Funding; Abbvie: Research Funding. Jakubowiak:Takeda: Consultancy, Honoraria; Amgen: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria; SkylineDx: Consultancy, Honoraria; Adaptive Biotechnologies: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria; Karyopharm: Consultancy, Honoraria; Celgene: Consultancy, Honoraria. Kaufman:Roche: Consultancy; BMS: Consultancy; Karyopharm: Other: data monitoring committee; Janssen: Consultancy; Abbvie: Consultancy. Mobasher:Genentech Inc: Employment; F. Hoffmann-La Roche Ltd: Other: Ownership interests non-PLC. Freise:AbbVie, Inc: Employment, Equity Ownership. Ross:AbbVie, Inc: Employment, Equity Ownership. Pesko:AbbVie, Inc: Employment, Equity Ownership. Munasinghe:AbbVie, Inc: Employment, Equity Ownership. Gudipati:AbbVie, Inc: Employment, Equity Ownership. Mudd:AbbVie, Inc: Employment, Equity Ownership. Bueno:AbbVie, Inc: Employment, Equity Ownership. Kumar:Oncopeptides: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; AbbVie: Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Research Funding; Merck: Membership on an entity's Board of Directors or advisory committees, Research Funding; KITE: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; KITE: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Membership on an entity's Board of Directors or advisory committees, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal